and Fasciotomy
Pathophysiology
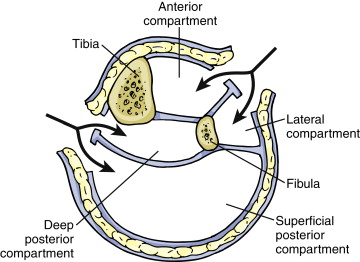
Osteofascial compartments
- three in upper arm, three in forarm, two in thigh, three in lower leg.
- envelope of fascia over muscle and bone
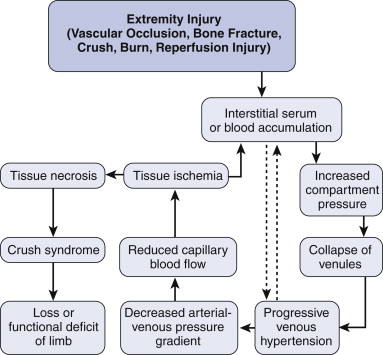
Viscous Cycle
Elevated tissue pressure within confined space leads to tissue ischaemia
--> decreased capillary perfusion
--> compression of venules causes venous hypertension; causes transudation into tissue space, worsening problem
--> worsening tissue ischaemia stimulates vasodilation, which leads to further fluid transudation
Compartment Syndrome
Beyond the local problem, true compartment syndrome is a systemic response.
- circulating inflammatory process; hyperkalaemia from cellular necrosis, ARF with rhabdomyolysis, acidosis.
Aetiology
Often crush injury, trauma; limb compression.
Burns, casts, splints,
Bone fractures, vascular injuries
Systemic - SIRS, sepsis, extravasation of IV fluids, ischemia-reperfusion injury.
Risk Fx
Popliteal vessel injury
Combined arterial / venous injury
Massive soft tissue injury; crushing
Prolonged ischaemia >4-6h
combined arterial, bone or soft tissue injury
Outcome
Depends on urgency treated, degree of irreversible tissue loss and necrosis
- peripheral nerves are more sensitive
PVD pts more prone to ischaemia
Shock and lib elevation reduce arteriovenous pressure gradient and worsen the problem.
Hypothermia and ice cause vasoconstriction, inhibiting perfusion further
Diagnosis
Pain, out of proportion to apparent insult,
- pain worse on passive stretch of compartment
Sensory and motor abnormalities, palpable tenderness / swelling, overlying skin change.
- sensory abnormality is an early change in significant compromise
Systemic features of hyperkalemia, acidosis and myoglobinuria.
Never rely on peripheral pulses or distal cap refil
- absent distal pulses mandate investigation for vessel injury.
Want the intervention to be before systemic features develop.
Direct measurement
Can measure with specificity
- Needle-catheter device on a syringe and manometer.
- Normal tissue pressures are 5-10mmHg
- Higher than this accompanied by compromise
- Up to 25-30mmHg requires intervention.
Management
Osmotic diuretics e.g. mannitol, ice packs, extremity elevation = probably all more harm than good.
Only effective therapy is fasciotomy
- as early and rapidy as possible.
Principles
Widely open compartments
Fully incise overlying epimysium and skin over entire length of incisions.
Avoid tight dressings, casts or splints
Osteofascial compartments
- three in upper arm, three in forarm, two in thigh, three in lower leg.
- envelope of fascia over muscle and bone
Viscous Cycle
Elevated tissue pressure within confined space leads to tissue ischaemia
--> decreased capillary perfusion
--> compression of venules causes venous hypertension; causes transudation into tissue space, worsening problem
--> worsening tissue ischaemia stimulates vasodilation, which leads to further fluid transudation
Compartment Syndrome
Beyond the local problem, true compartment syndrome is a systemic response.
- circulating inflammatory process; hyperkalaemia from cellular necrosis, ARF with rhabdomyolysis, acidosis.
Aetiology
Often crush injury, trauma; limb compression.
Burns, casts, splints,
Bone fractures, vascular injuries
Systemic - SIRS, sepsis, extravasation of IV fluids, ischemia-reperfusion injury.
Risk Fx
Popliteal vessel injury
Combined arterial / venous injury
Massive soft tissue injury; crushing
Prolonged ischaemia >4-6h
combined arterial, bone or soft tissue injury
Outcome
Depends on urgency treated, degree of irreversible tissue loss and necrosis
- peripheral nerves are more sensitive
PVD pts more prone to ischaemia
Shock and lib elevation reduce arteriovenous pressure gradient and worsen the problem.
Hypothermia and ice cause vasoconstriction, inhibiting perfusion further
Diagnosis
Pain, out of proportion to apparent insult,
- pain worse on passive stretch of compartment
Sensory and motor abnormalities, palpable tenderness / swelling, overlying skin change.
- sensory abnormality is an early change in significant compromise
Systemic features of hyperkalemia, acidosis and myoglobinuria.
Never rely on peripheral pulses or distal cap refil
- absent distal pulses mandate investigation for vessel injury.
Want the intervention to be before systemic features develop.
Direct measurement
Can measure with specificity
- Needle-catheter device on a syringe and manometer.
- Normal tissue pressures are 5-10mmHg
- Higher than this accompanied by compromise
- Up to 25-30mmHg requires intervention.
Management
Osmotic diuretics e.g. mannitol, ice packs, extremity elevation = probably all more harm than good.
Only effective therapy is fasciotomy
- as early and rapidy as possible.
Principles
Widely open compartments
Fully incise overlying epimysium and skin over entire length of incisions.
Avoid tight dressings, casts or splints