Primary
Survey
Principles
Airway & c-spine
Breathing &
ventilation
Circulation
Disability: neuro
Exposure / Environment
Adjuncts
Principles
Prehospital Preparation
Mobilise trauma team
Immediate transport to the closest best facility
Hospital Preparation
Ready equipment, eg airway gear, warmed crystalloid.
Warn lab / radiology.
Protect staff from communicable disease.
Triage
Sorti pts based on ABC priorities and resources available.
Multiple Casualties
Pts and injuries within facility's ability to render care.
Treat life-threatening problems and the multiple-system injured
first.
Mass Casualties
Number of pts and severity of injuries exceeds capability of
facility.
Treat those with greatest survival chance and least expenditure of
time first.
Primary Survey
Assess patients strictly order of ABCs
- Airway kills fastest, then breathing, then circulation
Assessment, establishing of treatment priorities and resuscitating
vital functions.
Life threats identified and treated simultaneously.
Same system for all ages, but:
- remember children lose heat quickly, have different dose
requirements and injury patterns.
- remember elderly have less reserve, comorbidities and medications.
- remember to establish pregnancy status early.
Transfer Needs
As primary survey and resuscitation progress, the need for
transferring the pt to another facility may become apparent.
Airway & C-spine
Ascertain patency
If communicating verbally, immediate jeopardy unlikely.
Establish patency
Maintain c-spine protection
- assume injury in any pt with multis-ystem trauma, esp if
above-clavicle injury or decreased GCS.
Chin lift / jaw thrust.
Use inline immobilisation if immobilising devices need to be
removed.
Inspect
Foreign bodies
Facial / tracheal / laryngeal fractures
Consider severe head-injury
Or altered LOC
Or GCS <8
Then usually place a definitive airway
- need is strongly suggested if nonpurposeful motor responses.
- maintain c-spine protection.
Secure the airway
Secure if potential for compromise
- nasopharyngeal airway may establish / maintain patency in the
conscious
- oropharyngeal if no gag.
If there is any doubt about
the patients ability to maintain their airway integrity, place a definitive airway.
- ie intubation or cricothyroidotomy if necessary
- temporary jet insufflation as a temporizing method in airway
emergency.
Frequent re-evaluation
There is potential for progressive airway loss; re-evaluate the
airway frequently.
Pitfalls
Equipment failure
Tube leak
Pt factors eg obesity, paralysis
Unknown laryngeal # / incomplete upper airway transection
Breathing & Ventilation
Examine
Expose the neck and chest
- inspect for rate/depth of resps
- inspect/palpate for tracheal position, chest movement, accessory
muscle use, injury.
Percuss for dullness, hyper-resonance
Auscultate bilaterally
Major Impairments / Immediate Life
Threats:
1. Tension pneumothorax
2. Flail chest
3. Pulmonary contusion
4. Massive haemothorax
5. Open pneumothorax
Lesser Impairments:
Simple pneumo or haemothorax
Fractured ribs
Pulmonary contusions
Manage
ventilation
Every pt gets supplemental O2 by mask / rebreather.
Bag-valve-mask ventilate if required.
Alleviate tension pneumothorax, seal open pneumothorax.
Intubation establishes definitive control of the pt with ventilatory
problems.
- a surgical airway should
be performed if oral / nasal contraindicated or cannot be
accomplished.
- beware ventilating a tension pneumothorax.
- attach a CO2 monitor to the endotracheal tube.
Pulse oximetry is valuable.
Pitfalls
Intubating a pt with tension pneumothorax.
Intubating may unmask or aggravate pneumothorax - reevaluation and
CXR after intubation is essential.
Circulation & Haemorrhage
Control
Haemorrhage is the predominant cause of preventable postinjury
death.
Within seconds evaluate:
1. Consciousness level
Due to poor cerebral perfusion.
Non-sensitive / late.
2. Skin colour
Pink extremities rarely goes with critical hypovolaemia.
Ashen skin / white extremities are ominous.
3. Pulse
Central (carotid or femoral).
Full slow, regular usually mean normovolaemia (watch for B-blockers)
Rapid, thready usually means hypovolaemia (not sensitive).
If absent with no local cause, take immediate resuscitative action.
4. Sources of bleeding
External and internal
Management
Control bleeding
Direct manual pressure.
- pneumatic splinting devices if available.
- do not use torniquets
(unless for amputation - crush tissue and provoke ischaemia)
- haemostats are too slow.
Recognised possibility of occult blood loss: thoracic / abdo
cavities, long bones, retroperitoneal from a pelvic #.
- obtain surgical consult.
NOTE: RECENT EVIDENCE SHOWS:
1. Excessive crystalloid prior to
hemorrhage control is harmful
--> dislodges clots, dilutes coagulation factors,
causes hypothermia
--> activates dysfunctional inflammation, worsens oedema (harm to
all organs), assoc. with abdo compartment syndrome
--> increased MOF, morbidity and mortality
2. Early high-ratio transfusion of plasma and platelets to RBCs
- 1:1:1 raio of these products
emerging as standard in wartime trauma
- civilian ratio: aim for 1.5 packed cells RBCs : 1 unit FFP
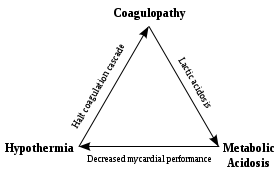
Trauma-Induced-Coagulopathy
There is an inappropriate
over-activation of protein C in severe trauma / bleeding,
causing an excessive anti-clotting response
- prompted by endothelial damage activating protein C
- causes inactivation of clotting factors (Va and VIIIa) -->
major reduction in thrombin formation.
There is also hyperfibrinolysis
- due to activation
of the fibrinolytic system (native t-PA), hypothermia, acidosis,
metabolic changes.
Fluid replacement
2 large-caliber IV lines
- upper extremity preferred.
- flow relates to diameter to the
4th power, inversely to length, but not to vein size.
Draw blood for type, crossmatch, FBC, U&Es, BHCG.
Ringer's lactate is preferred initial fluid (balanced)
- warmed to 39; max 1-2L then
blood
- beware lethal hypothermia from multiple transfusions.
Shock is usually hypovolaemic
- if pt remains unresponsive to IV bolus, use blood.
- non-matched type specific blood preferred to O -ve unless
unidentified casualties simultaneously treated.
Do not use vasopressors,
steroid, bicarb or continued fluids / transfusion - stop the
bleeding surgically.
In major bleeding, generally 4u blood then give 4u FFP (reassesses
blood needs)
- after ~6+ bags of blood start giving of platelets (really 6u) +
cryo.
- FFP contains II, VII, IX, X, XI
- cryo contains Factor VIII, fibrinogen and vWF, Factor XIII,
Fibronectin
Pitfalls
Carry an attitude of skepticism about volume loss.
- elderly may not increase HR & their BP has little correlation
with cardiac output.
- children have abundant reserve and show few signs until sudden
precipitous and catastrophic collapse.
- well trained athletes may not become tachycardic.
- unknown meds / comorbidities are possible.
Disability: Neurologic Evaluation
The priority after haemorrhage is neurologic status.
Establish:
Level of consciousness
- GCS is valuable and if not done here, do in secondary survey
Pupillary size / reaction
Lateralising signs
Spinal cord level
If LOC is altered (many
possible causes):
- Immediately reassess ABCs.
- Consider BSL.
- Consider alcohol, narcotics
- If these are excluded, consider it due to traumatic CNS problem
until proven otherwise, including post-ictal state.
Pitfalls
Frequent reevaluation is essential
- lucid intervals (talk & die) are possible with extradurals.
Return to the primary survey.
Exposure / Environment
Efforts to rewarm should
not be forgotten
- undress to facilitate full assessment.
- then cover them with warm blankets, use warming devices.
- remember to warm fluids and the room.
Log-roll.
Pitfalls
Some pts arrive already hypothermic.
Pts requiring massive transfusion become hypothermic
- best controlled by early haemorrhage control.
Adjuncts
Monitoring
HR, BP, pulse pressure, RR, ABG, Temp, pulse oximetry, urine
output etc
- obtain values and follow them ASAP after primary survey.
- periodically reevaluate.
Monitor exhaled CO2 with a colorimetric device.
Notes
Beware combative pts extubating themselves, deflating the cuff.
BP is a poor measure of tissue perfusion, especially in elderly.
Trauma triad of death
ECG
Monitoring
Attach all trauma pts to an ECG monitor.
Blunt cardiac injury may show rhythm, rate or ST disturbances.
PEA may indicate tamponade, tension pneumothorax, hypovolaemia.
Hypoxia and hypoperfusion may show as hypoxia and aberrant
conduction.
Hypothermia can produce dysrhythmia.
Catheters
Insert unless contraindicated
Urinary
Reflect renal perfusion, sensitive for volume status.
Contraindicated in urethral
transection.
- suspect if: 1) blood at meatus 2) perineal ecchymosis 3) blood in
scrotum 4) high-riding or non-palpable prostate 5) pelvic #.
Instead get a retrograde urethrogram first.
If anatomic difficulty encountered, consult urology early.
Gastric catheters
Decreases aspiration risk, decompresses stomach.
- does not prevent, and may actually induce vomiting on passage.
- ensure functional suction
on hand
- blood back may represent traumatic insertion, swallowed blood or
upper GI damage.
Insert orally if midface injury (suspected cribriform #).
XR and
Diagnostic Studies
Do not delay resuscitation
for XRs.
- defer to secondary survey time if required.
- do not avoid them in the pregnant pt.
Get AP chest, AP pelvis and Lat C-Spine.
- CXR may reveal life-threats
- Pelvic XR can indicate need for early blood transfusion.
- lat C-spine is useful if positive, but never excludes anything on
its own.
Consider DPL and USS abdo.
- can be compromised by obesity, bowel gas or DPL may be
under-sensitive.
Reassess