May be congenital and acquired
If acquired, may be infective, inflammatory, neoplastic (benign,
malignant; primary, secondary), trauma, degenerative.
Classification
Swellings superficial to the deep investing fascia are non-specific
to the neck.
Swellings deep to the fascia may be specific.
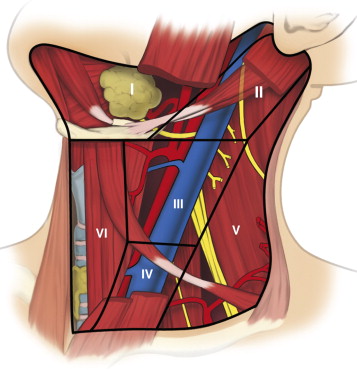
Deep swellings may be midline or lateral.
MANIFESTATIONS
A painless single enlarged node is a malignancy until proven
otherwise.
Other symptoms vary by cause.
Symptoms
Enquire as to cause.
- thorough systems review of all relevant structures.
Systemic features, e.g. fevers, sweats, weight loss, fatigue.
Signs
Site, size, shape, surface, edges, consistency, pulsatility,
mobility, fluctuance, pain, tenderness, lymph nodes.
- accurate site localization with knowledge of neck anatomy
- measure mass size accurately.
Key Points
Thyroid swellings move upwards.
Ventral lumps attached to the hyoid (eg thyroglossal cysts) move up
on swallowing and tongue protrusion.
Multiple lumps almost always lymph nodes.
Examine the full head and neck, including oral cavity.
Special attention to the aerodigestive mucosa, especially lymphoid
region of nasopharynx, base of tongue and oropharynx
Palpation includes bimanual exam of floor of mouth and neck to
identify abnormalities deep to normal mucosa.
Neurological exam of cranial nerves required.
Examine dentition
Reactive lymphadenopathy and primary, unusual or atypical
infections.
Perform:
Flexible Fibreoptic Laryngoscopy
- especially for patients with suspicious features / risk factors
Fundoscopy
Auroscopy
Nasopharyngoscopy
Bronchoscopy
Gastroscopy
FNA / biopsy. Allows rapid cytopathological diagnosis.
Must be done before any empiric therapy attempted.
- unless possibility of being vascular
Method:
- LA
- enter with slight negative pressure with a 20mL syringe and a 21g
needle
- hold mass in thumb and forefinger, use multiple angled passes
under negative suction; 3-4 aspirates
- reduce suction and remove syringe prior to removing the needle
from skin
- discard any blood
- squirt onto a slide, then that slide is smeared with a second
slide.
- promptly fix with ethanol or formalin before cells dessicate
--> best if a cytopathologist is on site to check specimen
adequacy
- sensitivity and specificity approach 90%, and are highest for
thyroid masses and solid carcinomas.
If nodes are cystic, need to biopsy the cyst wall with USS guidance
Imaging
USS first - accessible and no rads.
- cystic or not?
USS / CT often useful.
- contrast enhanced CT with fine slices of 3-5mm
MRI useful for soft tissue involvement or iodine allergies.
- may show certain lesions more accurate, e.g. carotid body
paraganglionomas
CXR in selected cases
- atypical infections and granulomas.
Role of PET Used for finding primary sources when endoscopies unhelpful.
Characterize extent of disease when previous known history of head
and neck malignancy.
- fusion PET/CT more useful tool; allows for accurate anatomical
localization of lesions.
--> accurate for occult cervical mets.
PET inappropriate when primary malignancy diagnosed.
- FNA the lesion
Broadly dependent on identification and diagnosis.
When infectious inflammatory, tissue diagnosis when ABx fail to
treat
When neoplastic, tissue diagnosis essential and thorough search for
primary source
- occasionally no identifiable primary; consider PET and MDT review
EUA Most lesions can be diagnosed in the clinic; in some, EUA is
useful
- e.g. if FNA unhelpful and clinical concern
Aids inspection of all mucosal surfaces
Biopsies under controlled settings
Medical Management
If <40, then medical management usually warranted in first
instance
Biopsy first in pts >40
Surgical Considerations
1. Many neck lumps are deep to platysma and may involve important
structures
- open biopsy under GA preferred
2. Incision lines in transverse relaxed skin tension lines
- should be sufficient to get safe exposure to important structures,
e.g. muscles, great vessles, CNs
3. Risks:
- neurovascular injury
- chyle leak
- nerves X, XI, XII at risk, as well as marginal branch of VII and
phrenic.
--> VII and XI most commonly injured Marginal branch of VII courses up from main trunk in parotid
to cross mandible and ultimate innervate lower lip depressors
-avoid region of body of mandible to reduce risk to this nerve; incisions
two finger-breadths below inferior edge of mandible CN XI exists in cranial base of jugular foramen
- passes over internal jugular as it travels to trapezius
- identify as it innervates SCM, if anterior border of digastric
skeletonized and fascia followed to SCM; n. is deep to posterior
belly of digastric.
- alternatively, along posterior of SCM about 2cm superior to Erb's
point; intersection of great auricular and posterior border of SCM
--> very superficial course in posterior neck, where easily
injured.
--> avoid cutting any structure passing through posterior neck
that is greater than 2mm CN XII passes levels I and II deep in the neck
- descends between IJV and carotid artery before innervating the
tongue musculature.
- surrounded by venae conniventes under posterior belly of digastric
--> may be damaged when controlling bleeding from the venae;
inadvertently clamped Thoracic duct lies in lower neck
- deep in inferomedial aspect of left supraclavicular region
- duct runs behind the common carotid and empties into the IJV near
its junction with the subclavian vein
- there are also chyle-containing lymphatics in the right neck that
should be controlled during dissection
- all tissue between phrenic and vagus should be dissected to avoid
a chyle fistula
--> manage chyle leaks with low-fat diet and medium-chain
triglicerides supplementation;
--> somatostatin may help to augment closure of a delayed chyle
leak
--> rarely, surgical intervention needed
4. Carotid body paraganglionoma
- high risk surgery; tertiary specialist job
- do not biopsy
- CNs at risk.
- usually achievable with subadventitial dissection and without
vascular reconstruction.